|
|

|
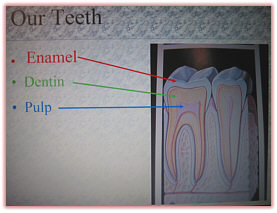
This website was created for the horse owner who wants to learn. For many, it will be the first time, perhaps, that they have ever heard of or considered any dental work for their horses. Considering the wide spectrum of knowledge that horse owners have, we wanted to lay a foundation to help the reader understand the reasons and the conditions that necessitate equine dentistry. A human tooth
is called a Brachydont tooth, defined as a short crown
tooth. That is our permanent tooth. Once it erupts and is in
place, that is all we get. We care for and use that same
short crowned tooth all of our life. The molars are
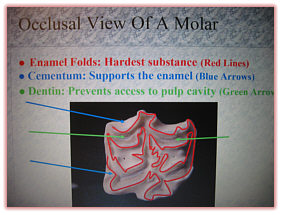
a combination of three substances, enamel, cementum and
dentin. Enamel, dentin and cementum are exposed on the
occlusal (chewing) surface of the tooth and wear at
different rates, therefore causing a permanent irregular
occlusal surface that is advantageous to the grinding of
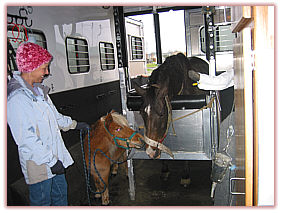
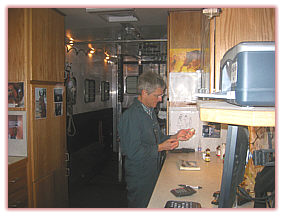
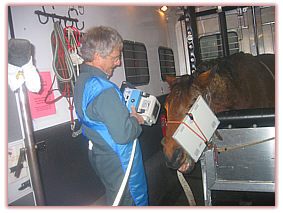
course fibrous food stuffs. We hope you will enjoy the website and the information it provides. Dr. Dick and Kathy Vetter. We work out of a 24' custom aluminum gooseneck trailer. It is 8'tall, 8'wide, double padded with the horse portion in the rear and the clinic portion in the front. We examine and treat horses in the trailer in a set of removable padded aluminum stocks. The majority of horses (90 - 95%) do walk in the trailer on their own as it is big and light and open. If need be, we can open it up even further. The horses are brought into the trailer and quietly sedated. If we do have a horse that is concerned about loading in the trailer, they are quietly sedated on the outside and then led in before the sedation totally takes affect. We have done thousands of horses in this manner. Advantages to our patients and clients:
** NOTE** Now that we have used the mobile clinic for over 3 years and several thousand horses, many of whom have been previously worked on by other practitioners, I am firmly convinced that a setting offering restraint and support, lighting, proper equipment and environmental control, offers a significantly higher level of practice. An experienced technician, who watches the horse closely, monitoring their sedation and comfort level, is also an invaluable resource to this practice. In my case, I am most fortunate that that person is also my best friend and wife, Kathy.
[ To Top ] We researched equipment for safety and efficiency. As there are many different procedures, angles, locations of teeth, and sizes of horses, we need specialized equipment to address those different jobs. We use a combination of power and hand tools. The equipment that we use to treat periodontal problems and tooth restorations has been adapted from human dentistry, with modified shafts to provide access to positions in the back of a horse's mouth.
**NOTE** We have run into some confusion regarding the ownership and use of "power tools" automatically equaling the expertise to use them correctly. Whether they are used by a veterinarian or a lay dentist (in some states), the horse owner needs to understand that the ownership does not necessarily make the operator an expert. It is a big responsibility to use a power tool correctly. The operator needs to have considerable instruction and experience, preferably under supervised conditions initially. That is difficult to find, unless one is dedicated to pursuing equine dentistry to the highest of levels. However, when they are used correctly, it is a positive to both the horse and the dentist, as a better job can often be done and in much less time. Correcting dental problems with hand floats, particularly if they are of a long standing nature, is very time consuming. It necessitates that the mouth is open longer, providing possible stress to the TMJ and also requiring repeated sedations to get the job done. We use a speculum to keep the mouth open when the horse is sedated. A speculum is an instrument with two bite plates that the front teeth rest on that is gently ratcheted open allowing manual and visual access to the mouth. It is attached to a leather halter. We use our head cradle to support the sedated horse's head. We want to keep him comfortable and accessible for us to work on his mouth in the most efficient manner. A plus to this is that the horses experience no fear or anxiety of this veterinary visit, as they are sleeping the entire time. Our practice philosophy is to offer the very highest in quality dentistry, from our pursuit of education to the equipment that we acquire. We have a computed digital radiographic unit that allows us to take both intra and extra-oral x-rays of the mouth and head. This technology has enabled us to expand our diagnostic capabilities dramatically. Periodontal disease, fractures, abscesses, extractions, can all be examined radiographically and definitive judgments made on the basis of better diagnostics. The following are a few examples where the digital radiography has been invaluable in correctly diagnosing a problem.
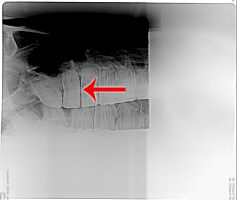
All radiographs are not "created equal". We often get a radiograph from a referring veterinarian, who might not have seen anything on the x-ray. They are usually correct, but not from a standpoint that there is nothing there, it is more likely that the "shot" wasn't a good one. A leg is basically composed of bones of similar density, creating a good contrast for interpretation. The horse's head is a myriad of varying densities of sinuses, bones and teeth that has long posed a difficult area of the horse to radiograph. This has often given the x-ray technician or veterinarian a challenge in getting an adequate image of the real problem. The benefit of having the digital x-ray capability on board with us is that we can take as many images as we need to zero in on the best angle and shot to identify the problem. We find that clients appreciate the opportunity to see their horse's radiograph and have the image explained to them. They also will have a copy made for them if they wish. Included in this section is an image of a periodontal pocket and an x-ray of the same, showing the spacing between the teeth and the loss of supporting tissue to the tooth.
Newborns to
one year old: Check incisor and molar alignment The newborn mouth should be checked primarily for a normal occlusion of the mouth. With the baby's head vertical, run a finger along the front of the gums/teeth to check if they are meeting evenly. If not, if one of the jaws is off, that is an indication that as those teeth come in, that baby will develop either an underbite or an overbite that will worsen when hooks develop that act as "braces" to exacerbate the problem. If the young horse's incisors have a tendency to not meet correctly, by the age of 3 months, he should be checked by an equine dentist. He may need to wear a mechanical or acrylic corrective device, such as a bite plate, for awhile to encourage a more desirable alignment. If he is not aligning correctly, he will also be developing small hooks that will add to the developing deviation. If you can catch these babies' little problems early enough, it can save bigger developmental problems in the future. I recommend that the first intraoral exam be performed at around 18 months of age. We usually find sharp enamel points and buccal (cheek) ulcerations at this time. We also find developing hooks on the 1st upper or lower deciduous cheek teeth that can have long term consequences on the developing skull structure. The two to
five year olds: This is a VERY important age to
be checking the mouth on a 6 month basis. Between the ages
of 2 and 5 years old, 24 permanent cheek teeth will erupt
with up to 16 teeth erupting simultaneously. When a young
horse loses a deciduous (baby) tooth, (often referred to as
a cap) some very sharp points are left behind on the
emerging adult premolar. This shedding process can cause
much discomfort as those sharp points can take 6 months to
smooth on their own. Those sharp enamel points often
lacerate the cheek. Deciduous teeth also become problematic
when they don't always shed on time. Retained caps can cause
delayed eruption (impaction) or malpositioning of permanent
teeth. We often encounter horses with training problems that are the direct result of their effort to avoid mouth pain. These training problems usually stem from current uncomfortable conditions in the mouth. However, aversion to past dental discomfort can become a learned behavior that becomes today's training problem. Either way, that horse is trying the only way it knows how, to avoid a stimulus that has caused it pain and often the rider is interpreting that behavior as resistance. There are many people who have changed bits, changed trainers and/or changed methods of training in an effort to find the fix. The fix was very possibly in their horse's mouth all the time. It is important
to remember that every experience our horses have,
particularly when they are young, is a training experience,
be it positive or negative. Being taught that the rider/bit
is something that hurts that young horse every time they are
present, can have negative consequences we'd rather
avoid.
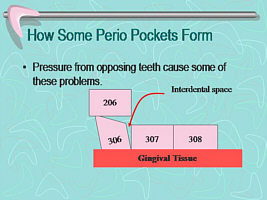
The dental problems that can become life threatening to an older horse, started years before when he was fat and sassy and his younger metabolism could compensate for some less than optimum dental/grinding/processing conditions. In some mouths that haven't had regular dental care, malocclusions (dental arcades, or rows of teeth, that haven't met efficiently) over long periods of time, have created significant gum and periodontal problems by now. Inflamed gums, loose teeth from periodontitis, possible absesses, broken and loose teeth, again from malocclusions, are all conditions that we find. Broken teeth are very painful for the horse. Loose teeth could be uncomfortable as they chew and also are the potential source of abscesses. When bad enough, they need to come out. Small animal and human dentistry have also documented that toxins released from infected (gum) tissue, do have a systemic affect on the heart and other organs, through bacterial release from infected gums and decaying teeth. These "bacterial showers" may initiate such conditions as endocarditis, kidney problems, etc In some mouths that haven't had regular dental care, malocclusions (dental arcades, or rows of teeth, that haven't met efficiently) over long periods of time, have created significant gum and periodontal problems by now. Inflamed gums, loose teeth from periodontitis, possible abscesses, broken and loose teeth, again from malocclusions, are all conditions that we find. Broken teeth are very painful for the horse. Loose teeth could be uncomfortable as they chew and also are the potential source of abscesses. When bad enough, they need to come out. Small animal and human dentistry have also documented that toxins released from infected (gum) tissue, do have a systemic affect on the heart and other organs, through bacterial release from infected gums and decaying teeth. These "bacterial showers" may initiate such conditions as endocarditis, kidney problems, etc. We personally have experienced dramatic changes in horse's demeanor and energy, when infections, either due to unknown severe periodontal disease or fractured and abscessed teeth, are diagnosed and treated. Systemic infections make horses sick! We might not notice the change, the lack of energy as it happens, but improvement is definitely notice when the infection is no longer in the body following treatment and resolution. An exam is done to the outside of the horse's face/head. The horse is under standing sedation. After deep enough sedation is achieved, a speculum is put in the horse's mouth, keeping it open and accessible (see Equipment). With a dental mirror and a dental pick, the gingival and periodontal health of the mouth is assessed, along with the condition and width of the interdental spaces. The infundibular area of the molars is checked carefully for possible decay. If treatment is necessary in any of those areas, it will be done following the equilibration of the mouth. (see Periodontics and/or Restorations) The premolars and molars are worked on first, visually sighting the arcades for balance. Slight imbalances of pressure can cause a tooth to fracture. The speculum is removed and the incisors are evaluated and treated. When all is done, your horse will be able to walk, albeit slowly. We normally recover them in a stall, but they can stand quietly with someone in a safe area. They will be coming out of the sedation quite well in 20 minutes, and ready to travel in an hour or less. We don't want them eating anything before that hour is up and/or they can chew and swallow efficiently. He may also be given an injection of phenylbutazone (Bute) an analgesic, depending on what was done in his mouth. Studies of equine athletes have indicated that going off of feed for even 24 hours, can change the pH of the stomach enough to predispose a horse to ulcers. He needs to be current on his tetanus, or will be given one at the time. We advise not riding him for 24 hours, perhaps 48. That time is dependent on the procedure done and the individual horse.
[ To Top ] Periodontics is the branch of dentistry that cares for the health of the tissues and ligaments that surround and support the tooth. Regular floating of your horse's teeth no longer constitutes comprehensive dental care as that technique does not address this area. Chronic advanced periodontal disease and infundibular decay are the leading causes of tooth loss in horses (and considerable discomfort). These are not newly discovered pathologies. What is new is our ability to treat them. Examination: What to look for A complete dental care session involves a thorough oral exam. Without a dental mirror a complete exam is not possible. With the dental mirror and a dental pick, the gums around and the spaces between teeth are carefully checked/probed as to the health of the tissue and/or the depth of inflammation/recession. Gingival inflammation and/or recession may be the first sign of low grade periodontal disease. Further examination can reveal gingival recession and often pocketing of varying depths (1 - 20 mm). Periodontal disease often exists in areas where seemingly harmless bits of feed are lodged between the teeth, often creating a foul odor. The odor is created by the feed that has been trapped in the enlarged interdental spaces, undergoing bacterial fermentation. Calculus or tartar buildup is another sign of progressing periodontal disease. Treatments:
Periodontal Disease The trapped feed needs to be removed before further damage is done. Our periodontal equipment is adapted from human dentistry. The only difference is the length of the shafts that allow access to treat interdental spaces and gingival areas that are as far back as the horse's eye. With this unit, the periodontal pockets can be cleaned and disinfected. A high pressure stream of prophy powder mixed with antiseptic dental solution dislodges all debris, removes bacteria and plaque as well as stimulates the inflamed soft tissues to begin the healing process. In cases of early detection, a single treatment has been found effective in restoring normal gingival margins. Periodontal pockets that are deep enough to warrant more aggressive therapy can be implanted with a flowable polymer that solidifies in the pocket. This implant then slowly releases an antibiotic into the surrounding tissues promoting regeneration of healthy tissue. This gel is slowly resorbed by the body. This process can also be repeated. Experience has shown most pockets respond with healthy gingival margins within two treatments. Occasionally, optimal healing can be achieved by combining systemic antibiotic therapy with the above procedure. The periodontal exam is included in our basic exam fee. If there is a problem found, the owner will be made aware of it and the extent of the infection/deterioration. If the periodontal disease is not of an advanced nature, equilibrating their mouth correctly alleviates the forces on the teeth that cause periodontal problems to occur. However, if the periodontal disease has progressed to the point that a tooth is in danger of becoming loose, it is highly recommended that the gingival tissue be treated at that time. This will reduce the infection and allow the gum and ligament an opportunity to more firmly attach to the tooth to hold it in place.
[ To Top ] Also of note during the initial exam should be the presence and the degree of any infundibular decay or open pulp chambers on any of the teeth. Early detection of both periodontal problems and infudibular decay is the key to saving the affected teeth. As mentioned earlier (see Introduction) the equine tooth is continually erupting. Enamel, cementum and dentin make up the tooth, giving different qualities of strength to its structure for the most efficient wear. In the infundibulum (center) of the tooth, occasionally the cementum is not "laid down" sufficiently, causing an area that is weaker and more vulnerable to decay. The decay starts on the central chewing surface of the tooth and eventually destroys and hollows out the core of the crown. Side to side chewing motions over this weakened crown can result in a longitudinal fracture that may often extend into the root structure. Tooth loss occurs as well as a possible sinus infection. Occasionally we
find a tooth that has an open pulp chamber. This may have
been the result of a fracture or mechanical over reduction
of a tooth. Often these are the first cheek tooth or the
canine. An exposed pulp chamber allows bacteria to invade
and infects the tooth with ultimate abscessation of the
tooth. When found, these need to be "capped" or sealed off
with a filling. Composite fillings are used which are cured with a curing light in the same manner as your own teeth are repaired. The composite filling is strong enough to withstand the grinding forces generated by the horse. The horse continually wears down the exposed crown. The composite filling will wear down at the same rate as the surrounding crown (generally 1.5 to 2.0 mm/year). The restoration
is done under the same standing sedation given to float the
teeth. The occasional decayed or fractured incisor can also
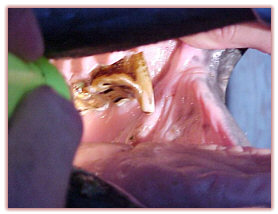
be drilled and restored in a similar fashion. If your horse's previous dental care has consisted of simply floating the teeth, it's very possible that other problems may exist. However, before those conditions can be treated they must be identified. To do a thorough exam, an equine dentist has to have the specialized training (your dentist does) to know how to identify these conditions. They also have to have the training to correct them and the specialized equipment to do it with. Preventing unnecessary tooth loss is much less expensive than the eventual cost of extraction and the maintenance of a specialized diet for a horse missing one or more cheek teeth, not to mention much less painful for the horse. Suze is an 18 year old Saddlebred mare. She was in good health, being ridden regularly and taken wonderful care of. A veterinarian had been treating her for four years for a nasal discharge. "Routine dentistry", intra nasal fiber-optic examinations and repeated courses of antibiotics had not "cured" the problem. Finally, the owner told him that she thought she might see a veterinarian who "just did teeth" ….. an equine dentist. His response was "don't waste your money". The owner came to us anyway and brought a horse that was in very good flesh and had a pleasant, quiet attitude. There was no outward indication of a problem. We sedated her and a thorough intra-oral examination revealed a severely decayed upper molar that had been missed every time her annual dental was done. It needed to be extracted. We normally do our extractions intra-orally. In her case, it had been decaying for so long that the internal structure of the tooth had "rotted" away, leaving no clinical crown to grasp with the extractors. Consequently, we had to refer Suze to a surgical facility. A pre-op x-ray showed a mass in her frontal maxillary sinus. As the surgeon lifted a flap of her skull to expose her sinus area, he discovered a huge inflammatory cyst along with a pocket of pus (that is the picture of the mass being held in the surgeon's two hands) The surgeon felt that this cyst was probably caused by the infected tooth that had been abscessing over the years. The mare healed
well and is now back on the trail with a profound increase
in energy. (The picture
shows a tooth in two pieces. The tooth was fractured in half
up the entire length of the tooth through the root and it
came out in those two pieces. The purple on the inside of
the tooth was a packing material that was used to get the
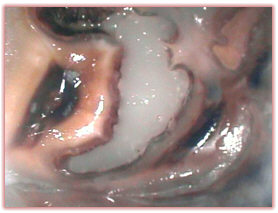
tooth out.) The picture shows the infected, painful periodontal pocket in between her teeth. The radiograph shows the space between her teeth where the supportive tissue is lacking.
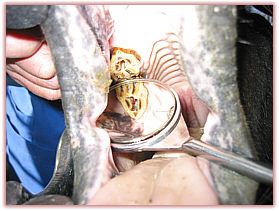
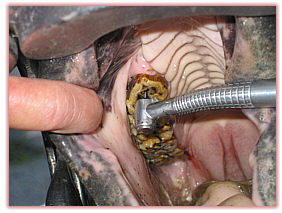
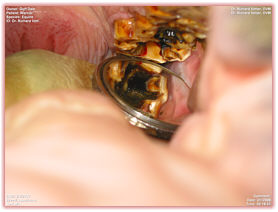
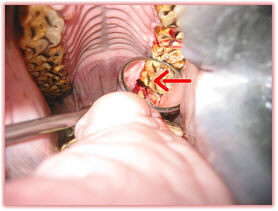
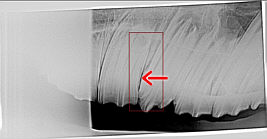
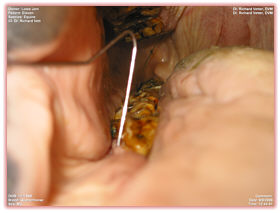
We saw Eleven in August. Upon examination, we found that he had not had his mouth balanced correctly over the years, and subsequently he had created some very deep periodontal pockets. (see Periodontal section) ** * The pictures below show the inside of Eleven's mouth with a dental probe indicating how deep that probe went into the infected pocket. The probe is 1 ¼ inches long. With the digital radiographic unit, we were able to take x-rays of Eleven's jaw to further diagnose his condition. The x-ray shows that the infection from the periodontal pocket involved the mandible (lower jaw bone) and if you look closely, you will see a difference in appearance of the infected bone. It looks "punky" compared to the line of bone further back. Not only that, but you will notice a curved line through the bone and that is where the bone was weakened by the infection and for what ever reason, broke. The jaw bone on this horse was broken, that is why he couldn't eat. And a likely reason for that could be traced back to infection from periodontitis, resulting from poor dental work over the years. The other picture shows a separation between teeth (we had already started to correct the mouth and the tall teeth had been taken down) and a gray "something" through the gum. That "something" is the broken jaw bone. The end of the
story is a happy one though for Eleven. We took the opposing
teeth back so that when he ground his teeth for any reason,
he wouldn't place pressure on the broken jaw area. He was
put on antibiotics to treat the infected gum and bone and
also he was instructed to have "horsey milk shakes" (Sr.
Feed and hay pellets, watered down to a gruel consistency)
for a while. Check ups and radiographs every several weeks
documented his recovery. His attitude, weight and condition
continued to improve and the jaw bone was healing. The first
of Oct., he went to Idaho to be with his girl and she is
back barrel racing him again. Her comment was that, when she
started to condition Eleven to put him back on the barrels,
she tried to take it slow and easy at first, but he got mad
at her, so off they went! People have told us that they think that having a dental done to their horse even if it isn't by a dentist, is better than doing nothing. That isn't particularly the case. When the wrong work is done, or incomplete work is done, that money would've been better spent if they'd found a good dentist in the first place (see FAQ, The Difference Between Equine Dentists and Veterinarians Who Do Equine Dentistry) Getting the teeth done by just anyone, often gives a false sense of the job being done and done well. It is so very important to not only know how to catch the occasional bad condition, but to examine and balance correctly the everyday dental exams so the painful and expensive conditions don't occur. CASE HISTORIES, 1996 - 2005
She had several premolar caps that hadn't come off completely. The retained caps and subsequent impacted molars were causing her a great deal of discomfort. One cap had twisted to the side and was still attached to some sensitive gum tissue. Under standing sedation, the caps were removed and the sharp points filed down to give her a smooth occlusal surface, no points jabbing her cheeks and she had a smooth and comfortable mouth again. The owner reported to us 10 days later, that she was given 3 days off, put back into training and was again the tractable filly that she had been.
The event horse
had been quidding a lot, we had thought that he had probably
lost a tooth and the feed was packing in the resulting
space. On examination, it was found that he had extremely
sharp points on the outside of his upper molars and the
points had ulcerated the insides of his cheeks so badly that
it was extremely painful for him to eat normally. He was
only able to eat if he packed hay into his cheek (the quid
that they saw) next to his ulcerations, and held it there as
a band-aid of sorts. Then he carefully ate his meal. Once he
learned his cheeks weren't going to hurt, he started eating
normally.
A 3 year old halter stallion prospect having his routine exam, was discovered to have a "parrot mouth" (overbite). He was presented to us for his 3 year old check-up for caps, points, and wolf teeth. Upon examination, we also found that the upper incisors were protruding over the lowers by approximately 1/2". He had hooks on the lower caudal (rear) molars and the upper rostral (front) premolars. The hooks were "trapping" the lower jaw back, exacerbating a tendency toward a parrot mouth condition, and making it worse than it genetically was. We took those hooks off, which allowed the lower jaw to move more freely, and the parrot mouth appearance, which was 1/2", became 1/8". If those developing hooks had not been removed, they would have acted like "braces", restricting the movement of the lower jaw and trapping it into a receding position that would have created a definite overbite or "parrot mouth" as a mature horse.
This horse had
been an easy keeper all of his life, until now. When we
examined his mouth, the first thing that was very apparent
was the long hook on the front of his first cheek tooth.
This hook definitely impeded his grinding motion and caused
him to have a shorter grinding stroke. It had also caused
unbalanced pressure on the opposing teeth. (see
Periodontics) When we treated this horse, we began by
reducing this long hook to the same level as the other teeth
in the arcade to help him chew/grind better. We also had to
remove the two teeth on the opposite arcade that had been
"worn out" and were loose, caused by the uneven pressure and
wear of the long tooth. That hook had not occurred
overnight, it was the accumulation of several years of
inadequate dental care. His owner was not aware of any
dental problems, as she was judging his dental condition by
his external appearance.
The two horses with the apparently stained incisors, on closer exam turned out to have serious defects involving loss of dentin and enamel. These probably had been caused by physical trauma such as a kick that then created a pathway for decay to ascend into the pulp cavity. Not only is this a source of ongoing pain for the horse, but the tooth will also be lost. Loss of a tooth causes the remaining teeth to shift and affects the balance of the entire mouth, requiring more frequent dental correction in the future. These horse's teeth were filled. (see Restorations and also Pictures) The filling itself will grow out with the tooth and wear off at the same rate as the tooth, taking about 5 years to disappear …… leaving a healthy tooth and not a gap. While debriding the decay in one of the horse's incisors, we found that decay continuing much further up into the pulp than we had anticipated. (It continued up under the gum.) This horse was profoundly sedated, and yet he was still wiggly, reacting to the discomfort of the depth of this decay. The (very competent) owners had had no idea this horse had a decayed tooth, as it only looked "discolored" before we started to repair it. One would have to assume that decay of this magnitude, was a source of ongoing discomfort to this horse on a day to day basis and nobody even knew it was there but him.
Performance Equine Dentistry Office: 360-829-0500, Cell: 360-508-0083, Fax: 360-829-0502 Email: vetent@centurytel.net Copyright © 2007 Performance Equine Dentistry, Inc. P.S. All Rights Reserved. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||